Diastasis is an increase in the distance between two sections of the rectus abdominis muscle. The separation occurs at the abdominal suture (Linea Alba and Linea Semilunaris) of the midline connective tissue in the anterior abdomen.
This phenomenon can occur after pregnancy, with rapid weight gain or loss, prolonged and significant physical activity, prolonged cough or regular constipation. The formation of diastasis is promoted by congenital weakness of connective tissue (dysplasia).
Diastasis is often combined with hernias of the anterior abdominal wall of various locations, varicose veins of the lower extremities, flat feet, hemorrhoids, blurred vision and scoliosis.
Strong and prolonged tension of the abdominal muscles leads to an increase in intra-abdominal pressure, and weakness of the linea alba leads to the fact that the muscles, under the influence of the increased intra-abdominal pressure created by them, begin to diverge to the sides. The so-called “vicious circle” closes when muscle tension causes a further increase in diastasis.
During pregnancy, under the influence of the hormone relaxin, the ligaments are stretched and the muscles of the anterior abdominal wall are weakened so that the uterus, and with it the abdomen, can expand with the growth of the fetus. After childbirth, the muscles gradually recover, but the tendons may remain in their previous state and create the appearance of a belly protruding forward.
In addition to a cosmetic defect, diastasis can be dangerous for a woman’s health, since a number of mechanisms that ensure the proper functioning of intra-abdominal structures, abdominal and back muscles are disrupted, and, as a result, pelvic discomfort and prolapse of internal organs may occur .
66% of women with diastasis of the rectus abdominis muscles note the development of urinary incontinence when coughing or sneezing, and discomfort during sexual activity. Diastasis and various pelvic disorders usually go hand in hand.
| 100% of women have some degree of diastasis recti in the third trimester of pregnancy, this means that physiological diastasis cannot be avoided, it is important to monitor the recovery afterwards. |
It is important to note that for many women, rectus discrepancy persists for 6-8 weeks after giving birth, and this discrepancy may remain unchanged for up to a year after giving birth. At the same time, a discrepancy of up to 2 cm is considered a physiological norm.
There are 3 degrees of diastasis depending on the size of the discrepancy of the rectus abdominis muscles:
1st degree – 2-5 cm; 2nd degree – 5-7 cm; Grade 3 – more than 7 cm.
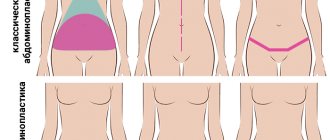
There are three types of diastasis depending on the location of the discrepancy:
- Above the navel;
- Below the navel;
- Mixed type (presence of muscle divergence both above and below the navel).
In 2009, a group of scientists conducted a study - using ultrasound methods, the width of the white line was measured in 150 primiparous women aged 20-45 years.
| It has been found that the average width of the linea alba can vary greatly, from 7 mm at the xiphoid process to 13 mm above the umbilicus and 8 mm below the umbilicus. |
Self-diagnosis of diastasis
If you suspect you have diastasis, we suggest you perform a self-diagnosis using video and record the results. To record, you can use the table in the infographic below or any medium convenient for you.
Diastasis is measured using three parameters:
- Divergence length
Measure how many centimeters the muscles extend up and down from the navel.
- Divergence width
How many centimeters are there between the muscles above the navel and below the navel?
- Finger depth
Evaluate how much your fingers sink when performing the test. During the recovery process, you will learn to engage the transverse abdominis muscle and the depth of immersion of your fingers during the test will become less.
During each test, observe the following aspects:
- Assess whether you experience pain in the pubic symphysis (the joint of the pubic bones).
- Try to feel the boundaries of the muscles along the middle of your abdomen and evaluate whether it is a soft tear or a clear separation of the muscles.
- See if you see a bulge or ridge.
- Listen to the sensations - do you experience discomfort in the pelvic floor area (involuntary release of urine, release of gases, air from the vagina).
| If something alarms you while performing these points, you should consult with your doctor to fully assess the condition of the abdominal cavity and/or pelvic organs before starting a cycle of exercises to correct diastasis. |
The video of the self-diagnosis test can be viewed below:
Loads with diastasis
The first thing that comes to the mind of a woman who discovers she has diastasis is to immediately start pumping up her abs. This is a fundamentally wrong decision.
| Classic abdominal exercises not only will not have a positive effect, but can also increase the separation of the rectus abdominis muscles. |
Research suggests that isolated abdominal exercises are not an effective way to combat diastasis .
A 2013 study published in The Journal of Strength and Conditioning Research identifies the following basic isolation and compound exercises that are recommended to be avoided for diastasis:
- lifting the body, legs, both together from a supine position; power crunches lying down, “bicycle”, “scissors”;
- yoga asanas that create strong pressure on the midline of the abdomen, such as Mayurasana and the like;
- power poses that significantly increase intra-abdominal pressure - power balances on the arms, swings and kicks, jumping, push-ups;
- poses that stretch or expand the abdominal wall - deflections, variations of bridges, including on a fitball or bench for deflections , pull-ups;
- straight planks;
- long stands on hands/elbows and knees/feet, such as push-ups.
| In everyday activities, you should avoid stress that leads to an increase in intra-abdominal pressure. Therefore, you have to think about redistributing household chores for a while. |
Please note a few important points:
- Wear a postpartum wrap when carrying your baby, especially if it lasts for a long time
- Do not carry weights weighing more than 5-6 kg . When lifting objects, bend your elbows rather than holding them at arm's length:
| Right | Wrong |
- Lie down and get out of bed on your side , as during pregnancy. Sleep on your back or side.
- If you need to get up from a chair , pull in your stomach and stand up mainly using the strength of your legs.
- Maintain correct posture: do not arch in the lower back, but do not slouch either.
Babywearing can also make diastasis worse. It doesn't matter whether you carry your baby in a sling, baby carrier, baby carrier, or in your arms, as long as you're violating your posture. It is poor posture in most women that causes pain in the lower back, thoracic spine, and pubic symphysis and provokes an increase in the degree of diastasis .
The main mistake many women make is rounding their backs, with their shoulders moving forward and the pelvis also moving forward - this compensates for the weight of the child by shifting the center of gravity, but significantly harms the health of the mother. In addition, the very weight of the child leads to an increase in intra-abdominal pressure, provoking an even greater divergence of the rectus abdominis muscles.
If you experience discomfort or pain while carrying a child, or you have grade 2-3 diastasis, you should stop using a sling during rehabilitation.
| If you are just planning a pregnancy, to prevent the development of significant diastasis, you should pay attention to strengthening the abdominal muscles, pelvic floor muscles, deep back muscles and diaphragm. |
During pregnancy, this will help support the growing belly, prevent pain in the lumbar spine and prevent prolapse of the pelvic organs. It has also been noted that with good development of deep stabilizer muscles, recovery after childbirth is much faster.
What causes diastasis? Causes of abdominal muscle diastasis
If you want to correctly adjust your body restoration program in the postpartum period, you need to understand the root of the problem and understand why the spatial arrangement of muscle structures has changed.
For reference, we mention that the development of diastasis is typical not only for pregnant women, but also for people who:
adhered to incorrect technique for performing exercises with heavy weights;- have an “apple” body type and have gained a lot of weight;
- suffer from the presence of dangerous abdominal fat (visceral);
- engage in sports that involve working with heavy weights (for example, powerlifting);
- suffer from chronic constipation, as well as a prolonged and strained cough.
During pregnancy, the active production of the hormone relaxin occurs, which is responsible for spraining the ligaments of the abdominal area. In this regard, the muscular muscles of the abdominal region weaken and intra-abdominal pressure gradually increases. The superficial and deep abdominal muscle groups are stretched, and the midline alba—the connective tissue tendon into which many of these muscles are woven—increases significantly in size.
Another reason for the increase in the size of the tendon line may be a congenital predisposition to poor connective tissue tone. This disease is called “dysplasia” - the occurrence of defects in fibrous connective tissue that occurred during the period of embryonic and post-embryonic development, which is due to genetic determination. This pathology is characterized by a defective state of the structures of collagen and elastin fibers, which form the basis of connective tissue.
Below we will figure out how to get rid of diastasis after childbirth.
Surgical correction
| Abdominoplasty is a surgical method for eliminating diastasis. For this purpose, tension plasty with local tissue or non-tension plasty with a synthetic mesh endoprosthesis are used. |
Current scientific evidence and clinical experience indicate that biomechanical and physiological causes, pregnancy and childbirth can affect the fascia of the abdominal support system, leading to diastasis. But not all women with diastasis recti require surgery to restore full function.
The current clinical hypothesis is that at least one year must pass after delivery before a decision can be made about the need for surgical correction of the dystasis.
| Finally, surgical intervention can only be indicated if a multi-tasking system for correcting dystasis, including nutrition, exercise and an active lifestyle, has proven ineffective for recovery. |
What is diastasis
Diastasis is a separation of muscle fibers along the midline of the abdomen, which can appear after pregnancy. According to statistics, it occurs in 25% of young mothers. Those women whose muscles are weak and untrained are especially susceptible to muscle divergence. Externally, diastasis appears as a protruding, “pregnant” belly. For example, it occurs in the third trimester and is normally observed until six to eight weeks after birth. If the muscles have not come together a year after giving birth, then you should not wait any longer; diastasis will no longer heal on its own. It must be dealt with, since the divergence of muscle fibers threatens with poor posture and the appearance of hernias.
To determine whether there is a muscle discrepancy, you need to see a doctor. You can do this yourself, but the diagnosis you make may not coincide with the real one due to your inexperience.
Depending on the width of the muscle divergence, several degrees of diastasis are distinguished:
- Degree 1 - muscle discrepancy from 5 to 7 cm. This defect has practically no effect on the shape of the abdomen. It is diagnosed more often in women after their first birth. Signs of diastasis of the rectus abdominis muscles at this stage are dull, low-intensity pain in the epigastrium, nausea, constipation, and bloating.
- Degree 2 - muscle discrepancy of more than 7 cm, in the lower section. At this stage, the abdomen is noticeable and protrudes, especially in the lower part. And also at this stage, relaxation of the lateral muscle groups is noted.
- Degree 3 - muscle discrepancy of more than 10 cm in both the lower and upper sections. This has a significant effect on the shape of the abdomen. At this stage, hernias (umbilical and linea alba) are common. In addition, more serious disorders are also worrying: muscle atrophy and even displacement of the abdominal organs.
The increase in the width of the muscle divergence depends on the degree of diastasis
Exercises to correct diastasis
It is important to note that the approach to correcting diastasis through exercise should be gradual and regular . Our system involves gradually engaging the deep core muscles to ensure an even load. As a result, this approach leads to the closure or significant reduction of diastasis.
| You can perform a set of exercises to correct diastasis in grades 1 and 2, in the absence of hernias and no earlier than 6 months after birth by cesarean section and 1 month after natural birth (start from the first stage of exercises). |
If you have grade 3 diastasis, you should stop at the first stage of the program until it reaches at least grade 2.
The #sekta diastasis rehabilitation program is conditionally divided into two stages:
- the first stage is the formation of a physical activity regime;
- the second stage is the transition to more intense exercises.
Work on correcting diastasis begins with correcting or strengthening posture, walking, joint exercises, normalizing diet, breathing exercises, strengthening the transverse abdominal muscle and pelvic floor muscles.
How does diastasis develop?
Diastasis has three degrees of development:
Stage 1 – from 5 to 7 cm;
Stage 2 – more than 7 cm;
Stage 3 – more than 12 cm.
Diastasis occurs not only in women, but also in men. Muscle separation is caused by either very strong strain or very weak muscles. And therefore, if a man was unprepared for stress and was exposed to it, then with very strong expansion, a discrepancy occurs. This is the first degree. If the first stage is easily corrected with the help of fitness, then the second stage can be corrected, but the muscles cannot be returned to their original place. In the third degree, only surgical method is applicable. In this case, our clients can contact the plastic surgeons of the Aesthetic City Plastic and Reconstructive Surgery Clinic, who will select the most effective way to eliminate diastasis. (More information about the clinic here).
If you want to fix everything, then you need to start with fitness. At any stage, if you work in the right direction with physical activity, the distance that determines the degree of diastasis decreases.
Correct posture
One of the most important, although at first glance insignificant, exercises is developing the skill of correct posture.
Over the course of some time, you will need to constantly monitor your body position: shoulders back, level above the pelvis, stomach moderately tucked, hips level, feet shoulder-width apart, toes spread for stability.
At first it will be unusual, but over time you will form the habit of standing and moving without disturbing your vertical position. Try not to tense your facial muscles, so as not to cause tension in your body. When moving your ribs and shoulders, you should not feel any discomfort in your stomach or hold your breath.
Make sure that your tailbone does not move forward and that your weight is distributed evenly without shifting to one hip - all these pelvic tilts indicate that the transverse abdominis muscle is not working. To engage the transverse muscle, pull your belly toward your lower back, concentrating on the area below your belly button.
An exercise near a wall will help you form the correct vertical position of your body: go to the wall, turn your back to it and press your heels, shins, buttocks, shoulder blades, shoulders and back of your head tightly. Having adjusted the position, perform 15-20 breathing cycles:
- On inhalation: the stomach relaxes, the ribs move to the side.
- As you exhale: we pull the stomach inward, only the abdominal muscles work, the shoulders do not move.
| Do this exercise at least 5 times a day in the first stage. It will take some time for your body to remember the correct muscle position. |
What to remember after an injury
Warm-up warm-ups before actual training will be very effective in reducing the likelihood of getting this injury in a sports environment. To do this, it is recommended to perform standard stretching exercises, warm-up jogging, etc. for 20 minutes.
In order to avoid sprains in everyday life, you need to calculate your strength when you have to do physical work with lifting weights. When performing it, it is recommended to take breaks and rest.
To maintain your muscles in tone and strengthen them, it is very important to give your muscles optimal loads on a systematic basis. You can, for example, visit gyms several times a week, do morning exercises, or go for daily jogging.
Breath
Breathing exercises help the diaphragm return to proper function after childbirth. During pregnancy, the diaphragm is pushed upward by the growing uterus and loses the ability to fully descend during breathing (inhalation phase).
The work of the thoracic diaphragm is closely related to the work of the pelvic diaphragm - they, like a vertical piston, always work together. Their well-functioning work has a beneficial effect on the functioning of all internal organs and the condition of the muscles of the anterior abdominal wall. Therefore, it is extremely important to set up this mechanism in a timely and correct manner.
To do this, you can use various breathing techniques:
1. Belly breathing.
Lie on the floor on your back, bend your knees, bring your knees and feet together, place one hand on your stomach, the other on your chest. As you inhale, gently inflate your stomach so that your hand on your stomach moves upward. As you exhale, gently lower your stomach down, pulling your pelvic floor muscles inward.
Try to prevent upward movements of the chest, controlling it with the other hand.
2. Lateral (costal) breathing.
Take a comfortable sitting position with a straight back, place your palms (all 5 fingers) on the lower ribs under the chest, point your elbows to the sides. Try “breathing into your hands” by pushing with the ribs of your palms, and feel the lateral expansion of your chest; The shoulders should remain motionless.
3. Alternating upper and lower breathing while sitting or lying down.
Take a position lying on your back, bend your knees, place your feet hip-width apart, parallel to each other.
Slowly begin to inhale, filling the stomach first and then the chest. When exhaling, push the air out first from the abdomen, then from the chest. As you exhale, additionally pull your stomach towards your lower back, direct the pubic bone towards the ribs (you can slightly twist the pelvis towards yourself and pull the pelvic muscles inward).
When to start exercising
To remove diastasis after childbirth quickly and effectively, you need to start training as soon as possible. Of course, you don’t need to do this immediately after discharge from the hospital - you should first wait until the lochia ends. Then the woman should monitor her condition a little.
So, in many women, diastasis goes away on its own a few weeks after childbirth. The maximum period for tightening damaged tissues is 1.5-3 months. If diastasis does not go away after this time, it means that it will not be possible to remove it without active action.
Important! You can perform exercises to get rid of diastasis no earlier than 4 weeks after giving birth!
Exercises to strengthen the abdominal muscles
Inclusion of oblique abdominal muscles, lateral bends, various variations of plank pose and specially adapted training for our students, taking into account increasing load from minimal to intense.
You can choose any 3-5 exercises and start with 10 repetitions on each side.
Side plank scissors, knee on the floor
Oblique abdominal muscles, back muscles, lateral thigh muscles, arm muscles.
Starting position (IP): lie on your side, support on your elbow, elbow strictly under your shoulder, supporting leg bent at the knee, back straight.
We lift the pelvis off the floor, the body is tense, from the shoulder to the knee - one straight line. Raise the straight left leg up, then lower it to the floor and lower the pelvis into the IP.
Side plank scissors
Oblique abdominal muscles, back muscles, lateral thigh muscles, arm muscles.
IP: lie on your side, support on your elbow, elbow strictly under your shoulder, legs straight, back straight.
As you exhale, lift your pelvis off the floor and lift your upper leg as high as possible. With an inhalation, we lower it and return to the starting position. IMPORTANT: do not lean to the side, the body is as tense as possible.
Side fold
Oblique abdominal muscles.
IP: lying on your side, the lower arm lies along the body, the other hand behind the head (elbow looking to the side). Legs are straightened, in the air, parallel to the floor (but do not lie on it!).
On the count of “one”, with an exhalation, we perform twisting to the side, trying not to just bend our legs at the knees, but to raise them as high as possible, reaching with our elbows towards our knees. The supporting arm bends at the elbow during twisting. On the count of “two” we return to IP. IMPORTANT: keep your feet on the floor throughout the entire exercise. We don’t lean forward or backward.
Dynamic side plank with forearm (knee on floor)
Oblique abdominal muscles.
IP: side plank from the forearm, the elbow is clearly under the shoulder, the supporting leg is bent at the knee 90 degrees and lies on the floor, the back is straight, the pelvis is twisted, the body is one straight line.
Slowly raise and lower your pelvis, tensing your abdominal muscles. IMPORTANT: the back is always straight, raise the pelvis as high as possible, try not to touch the floor at the lowest point, stop the pelvis 1-2 cm from the floor.
Dynamic side plank from forearm
Oblique abdominal muscles.
IP: side plank from the forearm, the elbow is clearly under the shoulder, the back is straight, the pelvis is twisted, the body is one straight line.
Slowly raise and lower your pelvis, tensing your abdominal muscles. IMPORTANT: the back is always straight, raise the pelvis as high as possible, try not to touch the floor at the lowest point, stop the pelvis 1-2 cm from the floor.
Pulling the knee to the elbow on all fours
Back muscles, arm and leg muscles.
IP: We stand in the “cat pose” on all fours: knees and hands on the floor, wrists strictly under the shoulders. We tear off the opposite arm (right) and leg (left) from the floor, stretch the leg back, arm forward so that they form one straight line with the back.
On the count of “one”, bend your leg at the knee, your arm at the elbow and pull the knee and elbow towards each other so that they meet under the stomach; when moving, the back is slightly rounded, the deflection in the lower back disappears. On the count of “two”, they extended their leg and arm to the IP.
Pelvic lift with leg lift
Gluteal muscles, back and front thighs, rectus abdominis muscles.
IP: lying on your back, arms along your body, both legs bent at the knees, feet on the floor. With an exhalation, we lift the pelvis upward. The body from the shoulders to the knees is in one straight line, supported by the feet and shoulders.
Without lowering the pelvis and maintaining a 90-degree angle at the knee, we pull the right leg towards the chest so that in the upper position the angle between the leg and the body is also 90 degrees. We return the leg to the floor, and inhale, lowering the pelvis. We repeat the same on the other side. IMPORTANT: when lifting the leg, the pelvis should not fall lower, keep it at the maximum level!
Video complex
At the second stage of rehabilitation, you can do exercises from our video complex:
The distance program presented by the #Sekta Ideal Body School for mothers contains detailed recommendations for reducing diastasis, a wide range of exercises and support from specialists. In this article we shared only a small part of our knowledge and gave a vector of work. This is not an instruction for action, but a basis for developing a plan to combat such an unpleasant problem .
Women are a great force, they generate love every second: for their husbands, for their children, for themselves. In our time, it is more important than ever to have a healthy body and soul so that the perpetual motion machine of love works without interruption, so that mother is active and cheerful, has time to take care of herself, realize her potential, and lives in harmony with her body. Diastasis is not a death sentence, but a reason to competently build your training schedule, adjusted for existing features.
Achieving an aesthetically beautiful abdomen, strengthening the abdominal wall and avoiding complications associated with muscle separation are the goals that many women who take the #sektamama course set for themselves. And they all note progress, the severity of which depends on the efforts that each makes. Even many years of experience with rectus abdominis muscle discrepancy can be corrected well, often helping to avoid surgical intervention. Try and you will reach your goal!
Author: obstetrician-gynecologist Valeria Pushkina, Department of Women's Diseases and Reproductive Health at the National Medical Center named after. N.I. Pirogov
Literature:
1. https://dianelee.ca/article-diastasis-rectus-abdominis.php. 2. Lee DG 2004 The Pelvic Girdle 3rd edn. Elsevier SyntaxError. 3. Lee DG 2007 Clinical Reasoning and Pelvic Girdle Pain: Show me the Patient! In: Proceedings of the 6th World 4. Congress on Low Back and Pelvic Girdle Pain, Barcelona, Spain, p 27. 4. https://dianelee.ca/article-diastasis-rectus-abdominis.php#sthash.ACQZUzfw.dpuf . 5. https://www.befitmom.com/diastasis_recti.php. 6. https://www.physiotherapy-treatment.com/diastasis-recti.html. 7. Fit Healthy Moms. 3 Ab Exercises to Heal Diastasis Recti. Available from: https://www.youtube.com/watch?v=Q6SfiH2-TEQ. 8. MomsIntoFitness. Diastasis Recti Exercises 5 min Core Workout. 9. Lee D, Lee LJ, McLaughlin L 2008 Stability, continuity and breathing: the role of fascia following pregnancy and delivery. JBMT 12(4):333–348. 10. Lee D 2011 Chapter 6 Pregnancy and its potential complications. 11. Lee D 2011 The Pelvic Girdle – An integration of clinical expertise and research, Elsevier.